
Sirolimus Wound Healing Risk Assessor
Patient Profile & Surgical Context
Comorbidities & Factors
Risk Assessment
Enter data to assess
Clinical Recommendations
Imagine you are recovering from major surgery. Your incision is closed, but instead of knitting together smoothly, the edges start to pull apart. For patients taking Sirolimus, also known as Rapamycin, a common immunosuppressant used in organ transplants, this scenario is not just a nightmare-it is a documented risk. Sirolimus saves lives by preventing organ rejection, but it comes with a heavy price tag for your skin and tissues: it actively slows down and disrupts the body’s natural repair processes.
The relationship between sirolimus and wound healing has been a source of intense debate in medical circles for over two decades. While early studies painted a grim picture of inevitable surgical failures, recent data suggests the story is more nuanced. It is no longer about simply avoiding the drug; it is about timing, dosage, and patient selection. Understanding how this medication interacts with your body’s healing mechanisms can mean the difference between a smooth recovery and a complicated hospital stay.
How Sirolimus Blocks Natural Repair
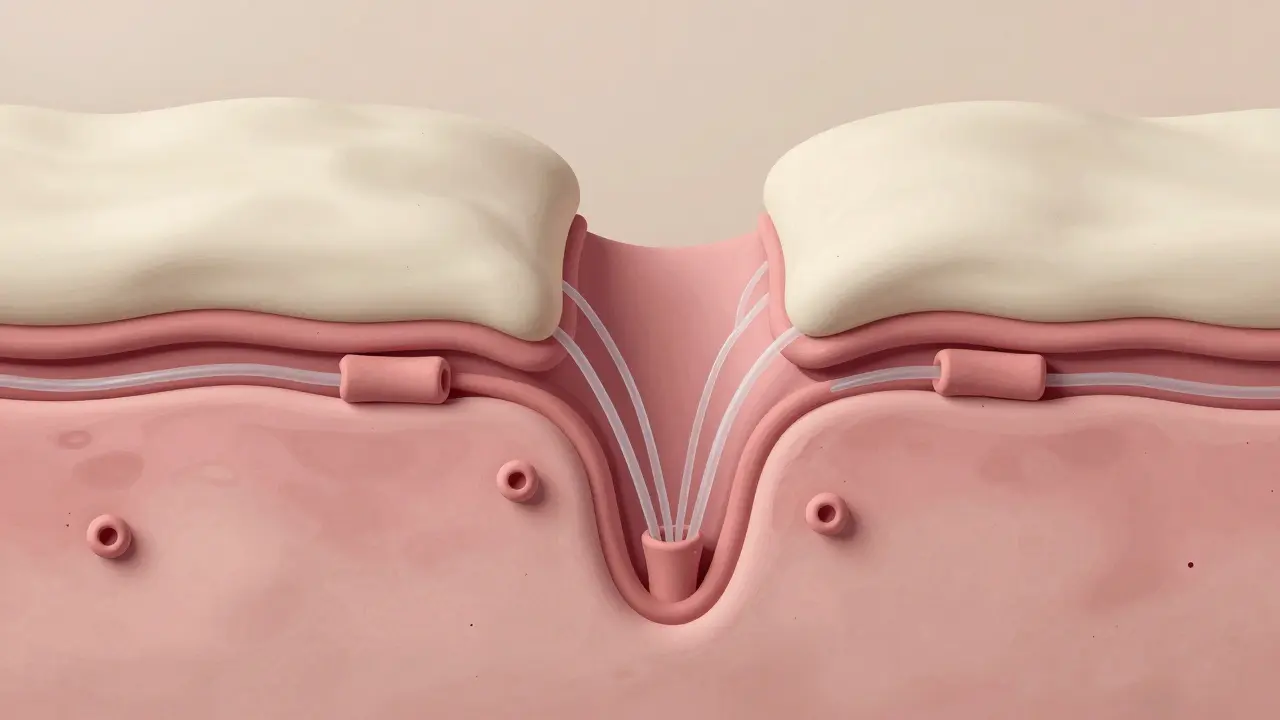
To understand why wounds struggle to heal on sirolimus, we have to look at what the drug actually does inside your cells. Sirolimus belongs to a class of drugs called mTOR inhibitors. The target, mammalian target of rapamycin (mTOR), is essentially a master switch that tells cells when to grow, divide, and multiply. By blocking this switch, sirolimus stops immune cells from attacking a new organ. But here is the catch: your body needs cell multiplication to heal a cut or an incision.
Research published in PubMed (PMID: 17384960) highlights a critical mechanism: sirolimus concentrations in wound fluid are often two to five times higher than they are in your blood. This local concentration bombards the healing site with inhibition. Specifically, the drug suppresses Vascular Endothelial Growth Factor (VEGF). VEGF is crucial because it signals the growth of new blood vessels (angiogenesis) needed to deliver oxygen and nutrients to the wound. Without adequate VEGF, the wound starves.
Furthermore, sirolimus inhibits the proliferation of fibroblasts and smooth muscle cells. Fibroblasts are the builders of your tissue-they produce collagen, the protein scaffold that gives strength to healing skin. Studies using rat models showed that therapeutic doses of sirolimus significantly reduced collagen deposition and decreased the breaking strength of wounds. In simple terms, the scar tissue forms, but it is weak and fragile, making it prone to dehiscence (opening up) under stress.
The Risk Factors: Who Is Most Vulnerable?
Not every patient on sirolimus will experience wound complications. The risk is heavily influenced by individual factors. A study led by Dr. Campistol emphasized that physical habitus plays a massive role. Patients with a higher Body Mass Index (BMI) face significantly increased odds ratios for wound healing problems. Why? Because larger body mass puts more mechanical tension on incisions, and adipose tissue (fat) has poorer blood supply compared to muscle, making it harder for healing factors to reach the site.
Beyond BMI, several modifiable risk factors compound the danger posed by sirolimus:
- Diabetes: High blood sugar impairs white blood cell function and circulation.
- Smoking: Nicotine constricts blood vessels, further reducing the already limited oxygen supply to the wound.
- Nutritional Status: Protein-energy malnutrition deprives the body of the raw materials needed for collagen synthesis.
- Uremia: Kidney dysfunction can lead to toxin buildup that interferes with cellular repair.
Dr. Saeed M. G Dawood’s team noted that except for age, most of these factors are modifiable. This means that preoperative optimization-stopping smoking four weeks prior, controlling blood sugar, and improving nutrition-can dramatically lower the risk profile before sirolimus even enters the equation.
Surgical Timing: The Critical Window
If you cannot avoid sirolimus due to its benefits for kidney preservation or cancer prevention, timing becomes your best tool. The consensus among many transplant centers is to avoid initiating sirolimus during the immediate postoperative period. The first week after surgery is the inflammatory phase of healing, where the body rushes cells to the site to clean debris and begin rebuilding. Introducing an anti-proliferative agent like sirolimus during this window is like putting the brakes on a car that is trying to accelerate out of a ditch.
Many clinicians recommend delaying sirolimus initiation until 7 to 14 days post-transplantation. This allows the initial structural integrity of the wound to establish itself. However, newer perspectives, such as those from Dr. Abdul Al-Ghamdi in a 2022 Wiley publication, suggest that blanket avoidance might be outdated. He characterizes earlier fears as "old myths" tempered by "new realities." With proper trough level monitoring, maintaining levels below 4-6 ng/mL during the first 30 days may minimize complications while still providing necessary immunosuppression.
The context of the surgery matters immensely. A large abdominal incision carries much higher risk than a minor dermatologic procedure. A study from the Mayo Clinic found that while infection rates were higher in the sirolimus group (19.2% vs 5.4%), the differences were not statistically significant in dermatologic surgeries. This suggests that for smaller, superficial procedures, the risk may be manageable even without delaying the drug.
| Strategy | Timing | Risk Profile | Best For |
|---|---|---|---|
| Immediate Initiation | Day 0-1 | High | Patients with high malignancy risk where immunosuppression is urgent |
| Delayed Initiation | Day 7-14 | Moderate | Standard transplant recipients with average BMI and good nutrition |
| Low-Dose Trough Monitoring | Day 0-30 (Levels <4-6 ng/mL) | Managed | Patients requiring early protection but needing careful wound surveillance |
Balancing Benefits Against Risks
Why do doctors prescribe sirolimus if it hinders healing? The answer lies in its unique advantages over other immunosuppressants. Unlike calcineurin inhibitors such as Tacrolimus or Cyclosporine, sirolimus is not nephrotoxic. It does not damage the kidneys. For long-term graft survival, protecting the kidney function is paramount. Additionally, sirolimus has antineoplastic effects, meaning it can help prevent certain cancers, which is vital for transplant patients who are at higher risk for malignancies due to chronic immunosuppression.
Approximately 15-20% of kidney transplant recipients receive mTOR inhibitors. The decision to use them involves a complex risk-benefit analysis. If a patient has a history of cancer or shows early signs of kidney toxicity from other drugs, the benefit of sirolimus outweighs the potential wound complication risk. The key is not to fear the drug, but to respect its mechanics.
Practical Steps for Patients and Clinicians
If you are a patient scheduled for surgery while on sirolimus, or considering starting it, communication is essential. Here is what you should discuss with your healthcare provider:
- Preoperative Optimization: Address any modifiable risks. Quit smoking, stabilize blood sugar levels, and ensure adequate protein intake.
- Timing Agreement: Ask if your sirolimus dose can be held or reduced for the first 7-14 days post-surgery. Do not stop medication without explicit instruction.
- Wound Care Vigilance: Expect stricter follow-up schedules. You may need more frequent dressing changes and checks for signs of dehiscence or infection.
- Trough Level Monitoring: Ensure your doctor is monitoring your blood levels closely to keep them in the therapeutic but safe range for healing.
Clinicians must also consider drug interactions. Other medications like steroids, mycophenolic acid, and antithymocyte globulin (ATG) also impact wound healing. Combining multiple agents that impair repair creates a synergistic negative effect. Simplifying the regimen where possible can reduce this burden.
Conclusion: Moving Beyond Fear
The narrative around sirolimus and wound healing has shifted from one of absolute contraindication to one of managed risk. While the biological mechanisms of impaired angiogenesis and collagen synthesis are real and significant, they are not insurmountable. By understanding the role of VEGF, respecting the importance of the first two weeks of healing, and rigorously managing patient-specific risk factors like BMI and diabetes, medical teams can harness the life-saving benefits of sirolimus without sacrificing surgical outcomes. The goal is not to avoid the drug, but to use it wisely, with precision timing and informed caution.
Does sirolimus permanently damage wound healing?
No, the impairment is temporary and related to the presence of the drug in the system. Once the drug is cleared or dosed appropriately, the body's natural healing processes can resume. However, if a wound dehisces while on the drug, it may require additional surgical intervention to close properly.
How long should I wait after surgery to start sirolimus?
Many clinicians recommend waiting 7 to 14 days post-surgery before initiating sirolimus to allow the initial inflammatory phase of healing to complete. However, this depends on individual risk factors and the type of surgery performed.
Can I take sirolimus if I have diabetes?
Yes, but with extreme caution. Diabetes is a significant risk factor for poor wound healing. If you are diabetic, your blood sugar must be tightly controlled before and after surgery, and your surgeon may delay starting sirolimus longer than usual.
What are the signs of wound dehiscence on sirolimus?
Signs include separation of the wound edges, drainage of clear or yellowish fluid, increased pain, redness, or fever. If you notice any of these symptoms, contact your healthcare provider immediately.
Is sirolimus better than tacrolimus for kidney protection?
Yes, sirolimus is not nephrotoxic, whereas tacrolimus can cause kidney damage over time. This makes sirolimus a preferred choice for patients with existing kidney issues or those at risk of long-term renal toxicity, despite the wound healing concerns.
Christina Mitchell
May 30, 2026 AT 10:15It is honestly fascinating how the body’s natural repair mechanisms are so delicate yet resilient. We often take for granted that a cut will just heal on its own, but this article highlights the intricate dance of biology at play. The fact that sirolimus can disrupt this process by blocking mTOR is a stark reminder of how interconnected our systems are. I appreciate the nuanced approach here rather than just saying avoid the drug entirely. It gives hope to those who need it for transplant survival while still acknowledging the risks. Timing really seems to be the key variable that we can control.
Cyburg Adeoye
May 31, 2026 AT 16:00As someone who has navigated the complexities of post-transplant care, I find the emphasis on preoperative optimization incredibly insightful!!! The mention of BMI and diabetes as compounding factors is something many patients overlook until it is too late!!! It is not just about the medication itself but the holistic state of the patient's body!!! We must educate ourselves on these modifiable risks because knowledge truly is power in medical contexts!!! Stopping smoking four weeks prior might seem like a small step but it could literally save your incision from dehiscence!!! Let us spread awareness about these critical windows of healing!!!
Joseph Teichman
June 2, 2026 AT 07:46good info. i had surgery while on rapamycin and my doc waited two weeks before starting it. wound healed fine. think timing is everything. dont skip meds without asking tho.
Angela Niculescu
June 2, 2026 AT 13:59I have to disagree with the idea that this is just about timing. The drug fundamentally alters cell behavior in ways that cannot be fully mitigated by waiting a few days. Many surgeons are too cautious and delay treatment unnecessarily, leading to other complications. The data cited here is selective and ignores cases where immediate initiation worked perfectly fine. It is time we stop treating sirolimus like a poison and start treating it like any other tool in the box. Fear mongering does no one any favors.
Victoria Mangiapane
June 3, 2026 AT 06:10Ugh another article making me feel guilty for existing?? Like yeah sure if you are fat or diabetic you are doomed but what about the rest of us?? It feels like every medical post ends with 'optimize yourself' which is just code for 'blame the victim'. My surgeon started me on day zero and I am fine so maybe the risk is overstated for normal people. Also why do they always use rat models?? Rats are not humans!!
Nivetha Narayanan
June 4, 2026 AT 11:43hey everyone! just wanted to say this is super helpful info! i know some ppl who are on sirolimus and they were scared to death about getting minor procedures done. knowing that low dose monitoring can help manage the risk is such a relief! lets support each other through these health journeys! stay positive and keep asking questions! 💖✨
Frank Arlyss
June 5, 2026 AT 23:51You guys are missing the point entirely. This isn't just about wound healing. It is about control. Who decides when you start the drug? Your doctor? Or do you have a say? I bet the pharmaceutical companies push for earlier initiation to maximize dosage adherence regardless of individual risk profiles. Think about it. They want you dependent. The whole narrative of 'managed risk' is a smokescreen to keep you compliant. Wake up.
Tim Reynolds
June 7, 2026 AT 16:47The VEGF suppression mechanism described here is textbook manipulation!!! Big Pharma knows exactly what they are doing!!! By inhibiting angiogenesis they are not just stopping rejection they are limiting your body's ability to fight back against their drugs!!! Look at the dates of these studies!!! They align perfectly with patent expirations!!! Do not trust the 'consensus'!!! It is all staged!!! Protect your kidneys but protect your truth more!!!
Groman Neta
June 9, 2026 AT 14:31This article is painfully obvious and lacks any real depth. Anyone with basic medical knowledge already knows that immunosuppressants impair healing. Listing BMI and diabetes as risk factors is redundant. It is elementary. The author fails to address the long-term psychological impact of living with this constant fear of wound dehiscence. It is a shallow overview that adds nothing to the discourse. Boring.
Ryan Jones
June 9, 2026 AT 19:45i mean look at it this way... why would they tell you to wait 7-14 days if not to cover their asses? probably because the drug interacts with something else they dont want you to know about. maybe the wound fluid concentration is higher because the body is trying to flush it out but the drug blocks that too. sounds fishy to me. i doubt the 'therapeutic window' is as safe as they claim. just my two cents but i dont trust the system.
Lisa Russo
June 11, 2026 AT 04:51Everyone here is overcomplicating it. Sirolimus stops cells from dividing. Wounds need cells to divide. Therefore wounds do not heal well. It is simple math. You do not need a PhD to understand that. If you are on this drug you should expect problems unless you are lucky. Stop looking for nuance where there is only biology. Just follow the instructions and hope for the best.
Michael Schurmann
June 12, 2026 AT 05:16It is quite amusing to see laypeople attempting to dissect complex pharmacokinetics with such superficial analysis. The interplay between mTOR inhibition and collagen synthesis is not merely a matter of 'timing' as suggested by the amateurish commentary above. One must consider the systemic inflammatory response and the specific isoforms of mTOR targeted. Without a robust understanding of cellular biology, these discussions remain trivial. Perhaps consult a peer-reviewed journal before offering unsolicited opinions.
Christopher Laver
June 12, 2026 AT 07:32Meh. Read similar stuff before. Nothing new here.
Russell Russell
June 12, 2026 AT 09:31We must remember that every challenge in our health journey is an opportunity for growth and learning. Understanding the mechanics of sirolimus allows us to take empowered steps toward better outcomes. Let us encourage one another to engage in open dialogue with healthcare providers. Knowledge is our greatest ally. Stay strong and informed!
Naresh Chandra
June 13, 2026 AT 00:24I deeply appreciate the detailed breakdown of the risk factors!!! It is crucial to recognize that healing is a multifaceted process!!! The emphasis on nutritional status resonates strongly with me!!! Protein intake is often neglected!!! We must prioritize our internal environment to support external repairs!!! Thank you for sharing this valuable information!!!